Last reviewed: May 2026 | Community resource — not medical advice. Surgical decisions should always be made in consultation with a dermatologist and surgeon experienced in HS.
For many people living with Hidradenitis Suppurativa, the conversation eventually turns to surgery. Maybe antibiotics have helped but not enough. Maybe a biologic controlled new lesion formation but left existing sinus tracts and scars that drain chronically and won’t heal on their own. Maybe the disease has progressed to a point where the affected area needs to be surgically removed to achieve any meaningful quality of life.
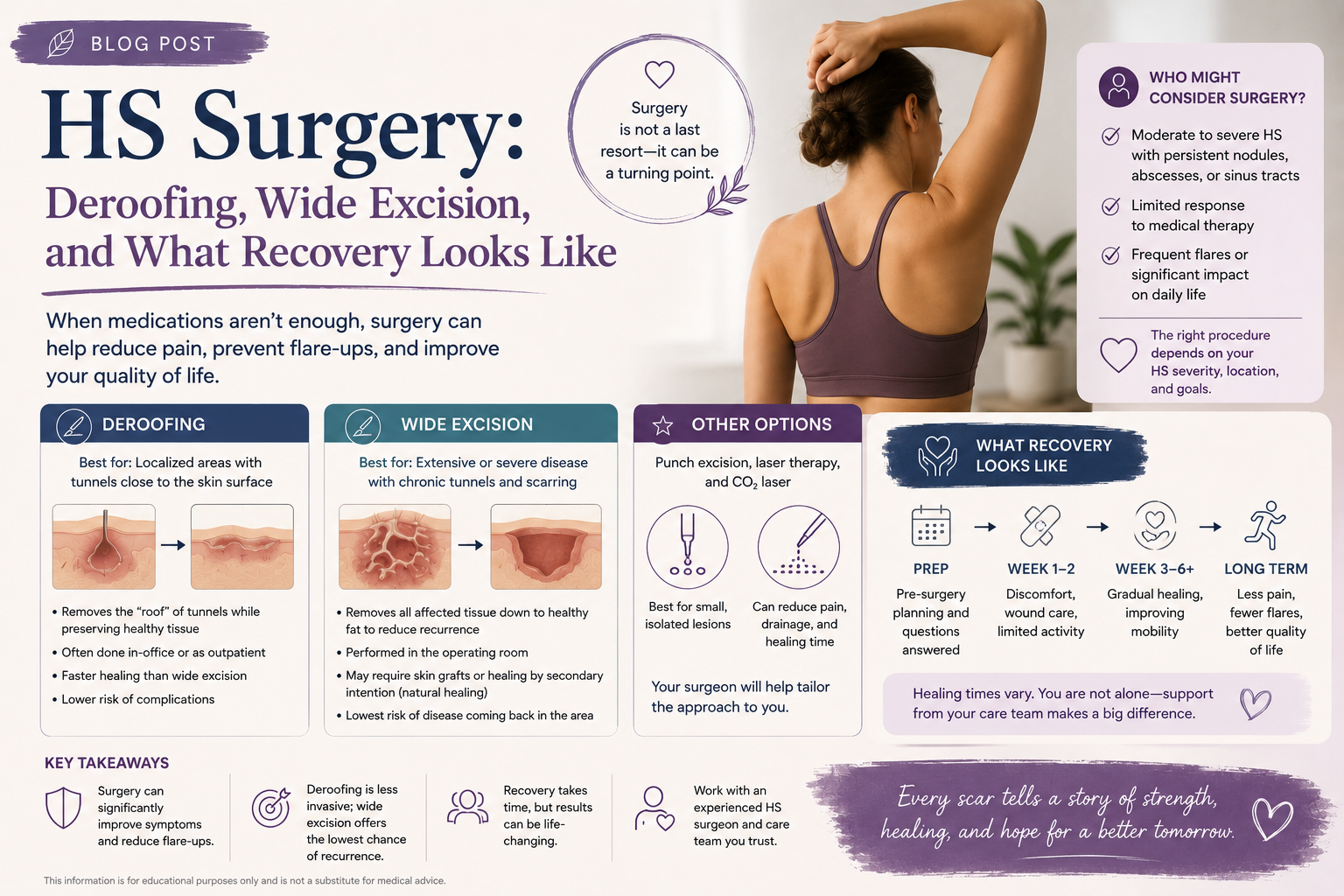
Surgery for HS is not a failure. It is not a last resort in the sense of something to dread. For the right patient, at the right stage, for the right body location, surgery can offer outcomes that no medication achieves — elimination of existing tunnels, removal of chronically inflamed tissue, and long periods — sometimes permanent periods — free of disease in the operated area.
This guide explains the main surgical options available for HS, what the evidence says about their outcomes and recurrence rates, what recovery actually involves day by day, how surgery and biologics can work together, and how to find a surgeon who genuinely knows this disease.
Why Surgery Becomes Necessary in HS
Medical treatments — antibiotics, hormonal therapy, biologics — work primarily by suppressing the inflammatory process that generates new HS lesions. What they cannot do is remove tissue that has already been destroyed.
Once sinus tracts (tunnels) have formed under the skin, they represent a physical structure — channels lined with epithelium, often filled with debris, bacteria, and inflammatory material — that medications cannot dissolve. These tracts can drain chronically, cause constant low-grade pain, produce odour, and act as a continuing source of inflammation that prevents surrounding skin from ever truly healing.
Similarly, established scarring and fibrotic tissue from years of repeated inflammation does not respond to immunosuppression. Surgery is the only tool that can physically remove these structures.
This is why surgery and systemic medications are not alternatives — they are complementary. Biologics reduce new lesion formation. Surgery deals with existing structural damage. The best outcomes in moderate-to-severe HS increasingly come from combining both.
The Surgical Options: An Overview
There are three broad surgical approaches used in HS, each with different indications, outcomes, and recovery profiles:
| Procedure | Best for | Complexity | Recovery | Recurrence rate |
|---|---|---|---|---|
| Deroofing (unroofing) | Individual tunnels, Hurley I–II | Low — often outpatient | Weeks (secondary healing) | ~17–27% |
| Wide local excision (WLE) | Larger affected areas, Hurley II–III | Moderate to high | Weeks to months | ~6–15% with good margins |
| Incision and drainage (I&D) | Acute abscess relief only | Very low — bedside | Days | Very high — not curative |
Let’s go through each in detail.
Incision and Drainage (I&D): What It Is and Why It’s Not a Long-Term Solution
Incision and drainage is the most commonly performed procedure in HS — and the least useful for long-term management. It is frequently what happens when an HS patient goes to an emergency department or urgent care clinic with a painful, fluctuant abscess: the doctor makes an incision, drains the pus, and sends the patient home.
This provides temporary pain relief. It does not treat the underlying lesion, does not address the sinus tract if one exists, and the lesion almost always recurs — often more quickly and severely than before, because the procedure disrupts the surrounding tissue without removing the source of the problem.
Current guidelines from both the US/Canadian HS Foundations and the European guidelines are explicit: incision and drainage is not recommended as a definitive treatment for HS. It may be appropriate as a bridge — to relieve severe acute pain while planning appropriate treatment — but it should not be mistaken for management.
“I had the same abscess drained at the ER four times over two years before anyone mentioned deroofing. Each time it came back within weeks. The deroofing worked and I haven’t had it come back in that spot since.” — HS Warriors member
Deroofing (Unroofing): The Tissue-Sparing Surgical Option
What it is
Deroofing — also called unroofing — is a tissue-preserving surgical technique in which the overlying skin (the “roof”) of a sinus tract, abscess, or cyst is removed, exposing the floor of the lesion. The floor is left intact, and the wound heals from the bottom up through a process called secondary intention healing — the body gradually fills in the open space with new tissue.
It is the right surgery for: individual or grouped tunnels in Hurley Stage I or II disease, lesions at specific fixed locations that have recurred multiple times, and patients who are not yet ready for or do not require wide excision.
How deroofing is performed
The procedure is most commonly performed under local anaesthesia in a dermatology clinic or outpatient surgical setting, though general anaesthesia may be used for larger areas or anxious patients. The steps, as described in clinical literature published in MDEdge (Cutis):
- The area is mapped — a blunt probe is inserted into the sinus tract to define its full extent and identify any communicating tunnels that aren’t visible from outside
- Local anaesthetic (usually lidocaine) is injected around the entire area to be treated
- The probe is used as a guide, and electrocautery or a scalpel is used to cut along the probe, removing the roof of the tract
- All connecting channels discovered during probing are unroofed in the same session
- The debris inside the tract — the keratin plugs, inflammatory material, and degraded tissue that accumulated — is removed with a curette
- The floor of the wound is left open — it is not sutured shut
- A non-adhesive dressing is applied, and the patient goes home with wound care instructions
The procedure typically takes 30–90 minutes depending on the number and extent of lesions. Most patients are able to go home the same day.
Healing after deroofing
Because the wound is left open, healing occurs over weeks to months depending on wound size. The original landmark deroofing study by van der Zee et al., published in the Journal of the American Academy of Dermatology, reported a mean healing time of approximately 14 days for the average defect of 3 cm in length — though larger or more complex deroofings take longer.
During healing, patients perform daily wound care:
- Gentle cleansing of the wound with mild soap and water once or twice daily
- Application of a moist non-adhesive dressing (typically a silicone or hydrocolloid dressing)
- Keeping the area covered and protected from friction and contamination
The healed result is typically a flat, stable scar — not perfect cosmetically, but in published patient surveys, the outcomes are consistently rated positively. In the van der Zee study, 90% of patients who underwent deroofing said they would recommend the procedure to others — a remarkably high satisfaction rate for any surgical procedure.
Recurrence rates after deroofing
The honest numbers: across published studies, recurrence rates after deroofing range from 14–27%. The landmark systematic review and meta-analysis published in the Journal of the American Academy of Dermatology estimated an average recurrence rate of 27% for deroofing specifically.
This means that roughly 70–83% of deroofed lesions do not recur in the treated area. When recurrence does occur, it is usually at the margins of the deroofed area — where the original probe didn’t fully map an extension of the tunnel — or in adjacent new disease, not a true failure of the procedure on the treated tissue.
📚 Reference: van der Zee HH et al. “Deroofing: a tissue-saving surgical technique for the treatment of mild to moderate hidradenitis suppurativa lesions.” JAAD, 2010. Read on JAAD
📚 Reference: Systematic review and meta-analysis of surgical recurrence rates. JAAD, 2015. Read on JAAD
CO₂ laser deroofing: an alternative technique
CO₂ laser surgery is increasingly used as an alternative to conventional electrosurgical deroofing. The laser acts as a precision cutting tool that vaporises the overlying tissue, provides simultaneous haemostasis (reduces bleeding), and has a mild bactericidal effect that may reduce infection risk.
A comparative retrospective study published in PMC in 2025 compared CO₂ laser deroofing versus surgical deroofing for HS tunnels and found the laser approach offered faster procedural speed, effective bleeding control, and reduced pain intensity compared to traditional surgery — with comparable recurrence outcomes. Most CO₂ laser procedures can be performed under local anaesthesia, avoiding general anaesthesia risks.
📚 Reference: “CO2 Laser Versus Surgical Deroofing for the Treatment of HS Tunnels.” PMC, 2025. Read here
Wide Local Excision (WLE): The Definitive Surgical Approach
What it is
Wide local excision is the surgical removal of the entire affected skin area — cutting down to the deep fascia (the fibrous tissue layer beneath the fat) and achieving clearance margins of 1–2 cm beyond the visible disease. The goal is to remove all affected hair follicles, apocrine glands, sinus tracts, and scarred tissue in a region, eliminating the source of disease in that area entirely.
WLE is the most appropriate surgery for:
- Hurley Stage II with multiple interconnected tunnels in a single anatomical region
- Hurley Stage III disease — diffuse involvement requiring removal of large areas
- Disease that has failed or recurred after deroofing
- Areas where ongoing drainage and infection are severely impacting quality of life
Surgical planning and staging
Wide excision for HS is frequently staged — meaning multiple surgeries are performed over time, addressing different anatomical regions in separate operations. This is deliberate and recommended. Attempting to remove all affected areas simultaneously would create too large a wound, carry excessive surgical risk, and make recovery unmanageable.
A retrospective study of 71 patients published in the Journal of Wound Care in 2024 found a mean of 3.7 surgeries per patient when treating multiple affected sites — confirming that multiple staged procedures are the norm for patients with widespread disease.
📚 Reference: Judge AC, Tahernia AH. “Hidradenitis Suppurativa: Radical Surgical Excisions with Staged Reconstructions.” Journal of Wound Care, 2024. PubMed
How the wound is closed after WLE
After wide excision, the surgeon faces a significant decision about wound closure. The options — and their recurrence implications — are meaningfully different:
Secondary intention healing — leaving the wound open to heal naturally from the bottom up, with daily wound care. Used frequently because it carries a lower recurrence risk than primary closure and avoids the complexity of grafting, but requires the longest recovery time (weeks to months depending on wound size).
Primary closure — suturing the wound closed directly. Fastest initial healing, but carries a higher recurrence rate (~15%) compared to flap or graft closure. Best suited for smaller defects with sufficient surrounding tissue.
Skin flap reconstruction — rotating or advancing adjacent healthy skin to cover the wound. More surgically complex, requires a plastic surgeon’s skill, but offers excellent outcomes: ~8% recurrence rate in the systematic review meta-analysis. Maintains tissue pliability and function. Particularly important for axillary (armpit) excisions where movement must be preserved.
Split-thickness skin graft (STSG) — harvesting a thin layer of skin from a donor site (typically the thigh) and applying it to cover the wound. Associated with the lowest recurrence rate (~6%) in published data, but has its own limitations: the graft site requires its own healing, and grafts in high-movement areas (axilla, groin) can develop contracture (tightening) that restricts movement over time.
Negative pressure wound therapy (NPWT) — a vacuum-assisted wound closure device that accelerates healing and reduces bacterial load. Often used as a bridge between excision and definitive reconstruction when the wound bed is heavily infected or not ready for immediate grafting. Research published in PRS Global Open in 2024 recommends 2–3 weeks of NPWT before secondary reconstruction in heavily purulent wounds.
The takeaway: flaps and grafts produce the lowest recurrence rates. If your surgeon is planning wide excision, it’s worth asking which closure method they plan to use and why — this choice meaningfully affects your long-term outcome.
📚 Reference: “Surgical Management of Hidradenitis Suppurativa.” Plastic & Reconstructive Surgery – Global Open, 2024. Read here
Recurrence rates after WLE
Overall recurrence after wide local excision averages ~13% across published studies — significantly lower than deroofing (~27%) or local incision (~22%).
The range within WLE depends heavily on closure method and how radical the excision margins were:
- Primary closure: ~15% recurrence
- Flap reconstruction: ~8% recurrence
- Skin graft: ~6% recurrence
- Regional (wider) excisions vs. partial excisions: recurrence drops from ~26% with partial removal to ~5% with regional excision — confirming that adequate surgical margins are critical
The most important predictor of surgical success is getting adequate margins — removing all affected tissue, not just the most obviously inflamed parts. HS has a tendency to have subclinical disease extending beyond the visible lesions, and inadequate margins are the most common cause of recurrence.
Recovery: What It Actually Looks Like Week by Week
Recovery varies significantly depending on whether you had deroofing or wide excision, and what closure method was used. Here’s what to expect:
Recovery after deroofing
Week 1: The wound is open but shallow. Pain is usually manageable with over-the-counter analgesics after the first 1–2 days. Wound care twice daily: gentle wash, non-adhesive dressing. Light activities are usually possible within a few days, though the treated area should be kept dry and clean. Avoid submerging in baths or swimming pools.
Weeks 2–4: The wound gradually contracts and fills with granulation tissue (new healing tissue). The wound typically appears red, moist, and granular — this is normal healthy healing, not infection. The size visibly reduces week by week.
Weeks 4–12: Final healing and re-epithelialisation. The wound closes over completely, leaving a flat scar. At 3 months, most patients report minimal or no ongoing wound care. The healed scar is typically stable and does not restrict movement significantly.
Return to work: For sedentary work, 1–2 weeks is typical. For physically demanding work involving the treated area, 3–6 weeks.
Recovery after wide local excision
Recovery after WLE is more involved and varies significantly by wound size, location, and closure method.
Days 1–3 (hospital or home): Pain is more significant immediately post-surgery. Pain management usually includes prescription analgesia for the first few days. Wounds closed with sutures or flaps will have surgical dressings changed by a nurse or at a wound clinic. Grafted wounds require close monitoring to ensure graft take (the graft adhering and beginning to integrate with the wound bed).
Week 1–2: Restricted movement in the affected area is important to protect the wound. Axillary excisions: avoid lifting the arm above 90 degrees. Groin/inguinal excisions: minimise sitting in positions that stress the groin. Driving is generally not recommended for 1–2 weeks after major surgery.
Weeks 2–6: Gradual increase in activity as wound healing progresses. Skin graft recipient sites develop new vascularity and the graft firms up. Skin graft donor sites (typically the thigh) usually heal within 2–3 weeks with dressing changes.
Weeks 6–12 and beyond: Full healing of larger wide excisions may take 2–4 months or longer for secondary intention closures. NPWT devices, if used, are typically in place for 2–3 weeks and managed with regular nursing appointments.
Physiotherapy: For axillary excisions particularly, physiotherapy to maintain shoulder range of motion during and after healing is important and should be arranged proactively. Contracture (scarring that limits movement) is a risk that physiotherapy significantly reduces.
Important: Any wound care questions during recovery should go to the surgical team, not the internet. Signs of wound infection (increasing redness spreading from the wound edges, increasing warmth, fever, foul-smelling discharge) require prompt medical attention.
Surgery and Biologics Together: Better Than Either Alone
One of the most important developments in HS management over the past few years is increasing evidence that combining biologic therapy with surgery produces better outcomes than either approach alone.
A systematic review published in Dermatologic Therapy in 2024 (Issa et al.) found that combined adalimumab and surgical treatment showed an 11.3-point greater decrease in IHS4 severity scores compared to adalimumab monotherapy, and a 40% higher increase in quality of life scores (DLQI). This is a clinically meaningful difference.
The logic is straightforward: biologics control the systemic inflammatory process that generates new lesions, while surgery removes existing structural damage that medications cannot reverse. Together, they address both dimensions of the disease.
A randomised controlled trial specifically examining adalimumab combined with surgery versus adalimumab alone confirmed superior outcomes in the combination group, and this is increasingly reflected in treatment guidelines worldwide.
📚 Reference: Issa P et al. “Combined Biologic and Surgical Interventions for Hidradenitis Suppurativa: A Systematic Review.” Dermatologic Therapy, 2024. Read on Wiley
Timing of biologics around surgery
A practical question: should you continue your biologic before and after surgery?
The current evidence-based position, supported by the SHARPS randomised clinical trial published in JAMA Surgery in 2021, is that adalimumab can be safely used in conjunction with HS surgery without significantly increasing surgical complications. Stopping biologic treatment around surgery — which many non-specialist surgeons instinctively advise based on protocols from other conditions — may not be necessary or beneficial for HS patients.
This is an important conversation to have with both your dermatologist and your surgeon. They should ideally communicate with each other rather than giving conflicting advice.
Factors That Affect Surgical Outcomes
Not everyone has the same surgical outcomes. Research identifies several factors that influence success rates:
Surgical margin adequacy — the single most important factor. Wider, more radical excision is consistently associated with lower recurrence. Conservative surgeons who try to save tissue often leave disease behind.
Smoking — active smokers have higher recurrence rates after surgery across multiple studies. Quitting before surgery improves healing and long-term outcomes.
Obesity — higher BMI is associated with more complex wound healing and higher complication rates, though some studies have found it does not independently predict skin graft need.
Hurley stage — Stage III disease has more extensive subclinical involvement, making adequate margin assessment harder and recurrence rates generally higher.
Body location — the perianal/perineal region and groin are technically more challenging and have higher complication rates than axillary surgery.
Continuation of systemic therapy post-surgery — maintaining biologics or antibiotics after surgery significantly reduces the risk of new lesion formation in adjacent areas.
Finding the Right Surgeon for HS
This deserves its own section, because the surgeon’s experience with HS specifically matters enormously.
HS surgery is not routine surgery. The disease behaves differently from other skin conditions — the extent of subclinical tunnelling is often larger than it appears on the surface, the tissue is chronically inflamed and often poorly vascularised from long-standing disease, and the anatomical locations involved (axilla, groin, perineum) are surgically challenging.
A surgeon who is unfamiliar with HS may:
- Underestimate the required surgical margins
- Not use a probe to map tunnel extent before excision
- Advise stopping biologic therapy unnecessarily
- Choose closure methods that maximise cosmetic outcome rather than minimise recurrence
Who performs HS surgery varies by country:
- In the US, HS surgery is performed by dermatologists (for deroofing), general surgeons, and plastic surgeons (for wider excisions and reconstruction)
- In the UK and Europe, HS specialist centres increasingly involve multidisciplinary teams with dermatology, plastic surgery, and colorectal surgery (for perianal involvement)
How to find an experienced HS surgeon:
- Ask your dermatologist for a referral specifically to someone with HS surgical experience — not just any plastic surgeon
- The HS Foundation provider directory (US) includes some surgeons
- The European Hidradenitis Suppurativa Foundation (EHSF) maintains a list of specialist centres in Europe
- The HS Warriors community forum has a regional dermatologist and surgeon recommendation thread with first-hand recommendations from patients
Questions to ask a potential surgeon before agreeing to a procedure:
- “How many HS excisions or deroofings have you performed?”
- “What margins do you typically aim for?”
- “What closure method do you recommend for my situation, and why?”
- “Do you work with a dermatologist who manages the medical side of my HS alongside surgery?”
- “Should I continue my biologic before and after the procedure?”
A surgeon who becomes defensive at these questions, or who cannot clearly answer them, is worth getting a second opinion on.
What Surgery Cannot Do
In the interest of honesty, here is what to understand before consenting to HS surgery:
Surgery treats the area operated on — it doesn’t treat HS systemically. New disease can and does develop in adjacent or new anatomical regions after surgery. Surgery in the right armpit doesn’t prevent disease in the left armpit, or in the groin. This is not a surgical failure — it is the nature of a systemic inflammatory disease.
Deroofing has a meaningful recurrence rate. Around 1 in 5–4 deroofed lesions will recur, typically at the margins. When that happens, the deroofing can be repeated. Most patients who experience recurrence still report they would have the procedure again.
Wide excision leaves scars. Sometimes significant ones, particularly for large excisions or those closed with grafts. Depending on location, these scars can affect movement (contracture) or appearance. Discuss the likely cosmetic and functional outcome with your surgeon before proceeding.
Recovery is real. Wide excision requires weeks of wound care, restricted activity, and follow-up appointments. Have a support plan — someone who can help with wound dressings, driving, and daily tasks, especially in the first 1–2 weeks.
The HS Warriors Community
Have you had deroofing or wide excision for HS? What was your experience with recovery, wound care, and outcomes? Your first-hand knowledge is some of the most useful information in existence for someone trying to decide whether surgery is right for them.
👉 Share your surgical experience in the forum 👉 Find surgeon recommendations by region 👉 Join HS Warriors — free and anonymous
This article is for informational purposes only and does not constitute medical advice. Surgical decisions should always be made jointly with a dermatologist and surgeon who are experienced with HS, after a thorough discussion of your individual disease extent, goals, and the available options.
Sources & Further Reading:
- van der Zee HH et al. “Deroofing: a tissue-saving surgical technique for HS.” JAAD, 2010. JAAD
- Systematic review: recurrence after surgical management of HS. JAAD, 2015. JAAD | PubMed
- Judge AC, Tahernia AH. “Radical Surgical Excisions with Staged Reconstructions: 71 Patients.” Journal of Wound Care, 2024. PubMed
- “Surgical Management of HS.” Plastic & Reconstructive Surgery – Global Open, 2024. LWW
- “Factors Affecting Wound Healing after Wide Surgical Excision of HS.” PMC, 2024. PMC
- Issa P et al. “Combined Biologic and Surgical Interventions for HS: A Systematic Review.” Dermatologic Therapy, 2024. Wiley
- “CO2 Laser Versus Surgical Deroofing for HS Tunnels.” PMC, 2025. PMC
- “Surgical Approach to HS.” ScienceDirect, 2025. ScienceDirect
- SHARPS trial: Bechara FG et al. “Efficacy and safety of adalimumab in conjunction with surgery in HS.” JAMA Surgery, 2021.
- HS Foundation. Provider directory. hs-foundation.org
- European Hidradenitis Suppurativa Foundation. Specialist centres. ehsf.eu
- HS Patient Guide. “The Right Surgery for the Right Time.” hspatientguide.com
- American Academy of Dermatology. HS Clinical Guidelines. aad.org